 By now most of you have heard that the Biden Administration is making one billion rapid at-home COVID tests available to the American public. This is in response to criticism that the government is not doing enough to combat the pandemic, particularly in the area of testing. There have been widespread shortages of at-home COVID tests and episodes of price gouging, so this seems to be a step in the right direction. How do you get the free test kits, and what should you know about their use?  How to Order Free At-Home COVID Tests: The Federal Government’s new website to process orders is up and running. Each household is entitled to four free at-home rapid COVID tests. The site is easy to use. It took me less than five minutes to order my free tests. Simply log on to https://www.covidtests.gov/, and input your name and shipping address. The U.S. Postal Service will process and ship the tests to your home within 1-2 weeks. If you don’t have internet access you may order your free COVID tests at (800) 232-0233. The website is not able to handle orders from multiple households living at the same address, so there have been a few glitches. For those situations you may call the Postal Service help desk at (800) 275-8777, or file a service request at https://emailus.usps.com/s/the-postal-store-inquiry.  The initial rollout of free at-home COVID tests is limited to four tests per household in order to promote broad access to the limited supply. But there are other ways to receive additional COVID tests at little or no cost to you. The test kits are available at some community health centers, rural clinics, and some federal testing sites.  Private Health Insurers Mandated to Cover At-Home COVID Tests: As of January 15th private health insurers are required to fully reimburse for up to eight at-home rapid COVID tests per person, each month. The insurer will not be able to apply co-payments or deductibles, and there is no requirement for a doctor’s order or a clinical assessment. The government is incentivizing insurers to work with pharmacies and other outlets to provide the at-home COVID tests with no out-of-pocket costs to the consumer. For specifics on reimbursements and no-cost programs, reach out to your health insurance provider.  Which At-Home COVID Test Will I Receive: There are thirteen at-home rapid antigen tests approved for use by the FDA to detect COVID. Only an approved antigen rapid test kit will be made available through the free program, but you do not have the ability to request a particular brand. Here are the currently approved at-home COVID antigen tests:
These tests are fairly easy to use and results are available in 15-20 minutes. Antigen tests detect the presence of a specific viral antigen, which implies current viral infection. The test requires you to swab each nostril for a specified period of time. The swab is then inserted into a buffer solution which then comes into contact with a test strip containing antibodies. A colored line appears on the test strip if it detects the antigen, indicating a positive test for the virus.  Sensitivity of Rapid Antigen Tests: Based upon ongoing research studies, the FDA updated its testing guidance in December to indicate that the rapid antigen tests for COVID have reduced sensitivity to the Omicron variant. The PCR (Polymerase Chain Reaction) test remains the gold standard for the detection of all variants of the coronavirus. PCR tests are run in labs using sophisticated equipment, and the results may take several days to receive. Due to this delay, PCR is not a good screening tool for COVID. During a PCR test the genetic material from the virus is copied billions of times. This amplification allows even tiny amounts of genetic material from the virus to be detected. Therefore, it can detect the presence of the coronavirus even before the onset of symptoms, but also long after your symptoms subside and you are no longer contagious. For rapid antigen tests to be positive, there needs to be a high viral load. The viral load in most COVID patients is usually too low for the antigen test to detect until after the onset of symptoms, sometimes several days after. With the Omicron variant, people seem to be coming down with symptoms earlier in the infection, before viral loads are large enough to be detected by a rapid antigen test. This doesn’t mean that these tests don’t work, but it does mean that when and how the tests are used can impact results. If you test positive on a rapid antigen test, there is a high probability that you have COVID. But if you test negative, you may still have COVID. The two most recently approved rapid antigen tests show higher sensitivity to the detection of the Omicron variant than previous tests. These are the “Clinitest Rapid COVID-19 Antigen Self Test” by Siemens-Healthineers, and the “Standard Q COVID-19 Ag Home Test”, by SD Biosensor.  When to Use At-Home Rapid Antigen Tests: These tests are most accurate when you are symptomatic for COVID. The CDC recommends using an at-home test if you have a fever, cough, sore throat, respiratory symptoms, muscle aches, or lose of taste or smell, https://www.cdc.gov/coronavirus/2019-ncov/testing/self-testing.html#anchor_1638718975230. Rapid COVID tests are also recommended for use five days after a potential COVID exposure, and as part of test-to-stay protocols in schools and workplaces. For best results I would wait 2-3 days after the onset of symptoms before testing with a rapid antigen test. A positive test result indicates that you likely have a current infection, and you should isolate and inform close contacts. A negative test result indicates that you may not be infected and may be at low risk of spreading disease to others, though it does not rule out an infection. If you plan to visit a vulnerable person in the near future, such as your grandmother, plan ahead. Minimize your social contacts for about a week and take a minimum of two tests prior to your visit. The final test should be within 24 hours of your visit. If you are symptomatic and get a negative test, repeat the test after 24-48 hours. This type of serial testing is often required for an accurate result, but it becomes problematic when you have a limited supply of tests available. Never rely on a single negative test, particularly if you have symptoms. It is best to self-isolate and have a PCR test performed, or assume that you are positive and take the necessary precautions.  Other Considerations:
 The government is discouraging the use of cloth face-masks. The CDC has updated its face-mask guidance to emphasize the better protection offered by N95 and KN95 masks. The Biden Administration is making available 400 million N95 masks free of charge to the American public. The free masks will be made available through select pharmacies and community health centers. You can find a list of locations offering the free masks at this link.  The lack of adequate testing has hindered the United States’ response to the pandemic since day one. Most experts acknowledge that testing is an important step in mitigating virus spread. It appears as if the Biden Administration has finally determined that vaccines alone will not end this pandemic. The programs to provide free test kits and face masks to the American public are steps in the right direction. Now it’s time for every American to avail themselves of these tools and do their part to bring this pandemic to an end.  If you enjoy reading this type of commentary please subscribe to my blog and tell a friend. You will receive an email notification when new blogs are posted. The email will come from the site’s email: armchairamerican1776 @gmail.com.
Thanks, Armchair American
0 Comments
 On August 23, 2021, the Food and Drug Administration (FDA) granted full approval to the Pfizer/BioNTech COVID-19 vaccine for people age 16 and older. This vaccine had been authorized for emergency use since December 11th for people age 16 and older. In May the emergency use authorization was expanded to include children age 12-15, which still remains in effect. Of the approximately 170 million Americans who are fully vaccinated, about 54% received the Pfizer vaccine. The approval comes 97 days after Pfizer provided the FDA with over 340,000 pages of documents to support their application. The FDA had reportedly been working on the application around the clock, and the approval took about half the time that it normally does. Now that the Pfizer vaccine has received the FDA’s gold standard for safety, effectiveness, and manufacturing quality, will it provide the impetus for vaccine holdouts to get vaccinated? What are the other implications of the Pfizer vaccine approval, and what about the other COVID-19 vaccines?  Vaccine Holdouts: Public health officials are hopeful that the FDA approval of Pfizer’s vaccine will motivate more people to get the vaccine. As of August 23rd, there were approximately 82 million eligible Americans who had not yet received a COVID vaccine, for a variety of different reasons. According to the Kaiser Family Foundation, 3 in 10 unvaccinated adults said that they would be more likely to get vaccinated if one of the vaccines were to receive full FDA approval, https://www.kff.org/coronavirus-covid-19/poll-finding/kff-covid-19-vaccine-monitor-june-2021/. This is certainly encouraging, but only time will tell. It has been known for some time that a major reason for vaccine hesitancy is due to the notion that COVID vaccines are “experimental”. The FDA approval of the Pfizer vaccine takes this excuse off the table. 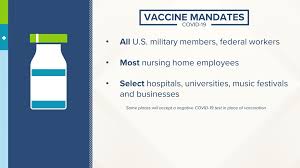 Vaccine Mandates: Mandating a vaccine that had not received full FDA approval was problematic from a legal and ethical standpoint. But that has all changed. On the same day that the Pfizer vaccine received full FDA approval the Pentagon announced that it would require all active-duty service members to be vaccinated. Many large employers, school districts, universities, and other public and private entities have also announced vaccine mandates in recent days. Many organizations and municipalities have tried to increase vaccination rates by offering prizes and giveaways, with limited success. Mandates might help to push some people who are still on the fence about getting vaccinated.  Other Implications of Full FDA Approval:
 Booster Shots are Coming: The Biden Administration prematurely announced that starting September 20, 2021 booster shots would become available for adults eight months after their second shot of either the Moderna or Pfizer COVID vaccine. But before this can happen each vaccine manufacturer needs to receive FDA approval to provide boosters for their particular vaccine. To date only Pfizer has provided the FDA with initial data to justify a booster shot. Pfizer plans to submit its full application within days to provide boosters to people age 16 and older. Moderna and Johnson & Johnson will submit their data later this fall.  Approval for boosters is not a matter of if, but when. The data coming in is overwhelmingly positive. This week Pfizer released data showing a third dose given 5-8 months after the second dose resulted in a 3- fold increase in coronavirus fighting antibodies, https://www.reuters.com/world/us/pfizer-starts-process-seek-us-approval-covid-19-vaccine-booster-2021-08-25/. Data coming out of South Africa shows a 9-fold increase in antibodies from a booster dose of the Johnson & Johnson vaccine given 6 months after the first, https://www.cnn.com/2021/08/25/health/johnson-vaccine-booster-data/index.html. If you can’t wait for the FDA to officially sanction booster shots, simply ask your personal physician. If you have been fully vaccinated with the Pfizer vaccine, your physician may legally provide a third dose now that it has received full FDA approval.  Vaccine Inequity: Not everyone is happy about the U.S. and other developed countries rolling out booster shots. The head of the World Health Organization called the strategy “a mockery of vaccine equity”. With only about 2% of the African population fully vaccinated, I tend to agree. We have seen how contagious the delta variant is. Unvaccinated people are the incubators of new coronavirus variants, which could one day overcome the protection offered by current vaccines. The full FDA approval of the Pfizer vaccine is a good thing. It legitimizes this important weapon against COVID-19, which is still rampaging through the world. It eliminates the stigma of being “experimental” used by many as an excuse for not getting vaccinated. FDA approval provides legal cover for businesses, organizations and schools to mandate COVID vaccines when they deem it necessary. In the weeks and months ahead, Moderna and Johnson & Johnson will be submitting applications for full FDA approval for their vaccines. COVID vaccines have saved countless lives and have been used safely in hundreds of millions of people around the world. Full FDA approval of these vital vaccines can’t come soon enough.  Here is a link to the FDA press release on the full authorization of the Pfizer COVID vaccine, https://www.fda.gov/news-events/press-announcements/fda-approves-first-covid-19-vaccine. If you enjoy reading this type of commentary please subscribe to my blog and tell a friend. You will receive an email notification when new blogs are posted. The email will come from the site’s email: armchairamerican1776 @gmail.com.
Thanks, Armchair American  The World Health Organization has identified vaccine hesitancy as a leading global health threat, which left unchecked could lengthen the duration of the COVID-19 pandemic. The United States is far ahead of most nations in vaccinating its population. But even the Centers for Disease Control and Prevention recognizes that reaching herd immunity is no longer a realistic goal. The best hope to mitigate the consequences of the pandemic is to get as many people as possible vaccinated, within the shortest period of time.  President Biden has a goal of getting at least 70% of the adults in the U.S. vaccinated with at least one shot by the 4th of July. This should be achievable, but it won’t be easy. To date about 64% of adults have received at least one COVID shot. But the pool of adults willing and able to get vaccinated is shrinking. Lack of access and misinformation are leading to vaccine hesitancy and outright refusal to get the shot. Lack of access to the vaccine in certain populations is a big challenge, but one that can be overcome with time and resources. Reaching the homeless, migrant workers, shut-ins, and isolated rural communities present logistical challenges. The more difficult challenge will be to overcome all the misinformation out there and get through to those refusing to get vaccinated.  Who is Hesitant about Getting Vaccinated: The Kaiser Family Foundation COVID-19 vaccine tracking poll tracks vaccination rates and behavioral attitudes towards vaccinations among various demographic groups, https://www.kff.org/coronavirus-covid-19/dashboard/kff-covid-19-vaccine-monitor-dashboard/?gclid=EAIaIQobChMI_qiK1aGI8QIVIPHjBx2Ejw5SEAAYAiAAEgJt2fD_BwE. Here is some of the latest data on adult vaccination rates in the U.S.:
The people in the last two groups, making up 20% of the adult population in the U.S., are considered “hesitant” about getting the vaccine. This hesitant group tends to be younger, Republican, and from rural communities. Here is the breakdown for these groups: Group Hesitant or Outright Skeptical Ages 30-49 28% Republicans 36% From Rural Areas 27% The most significant determinant among all groups, including race and gender, was the level of education. Working class members of every demographic group are less likely to be vaccinated and are hesitant to do so. People with a college degree are twice as likely to be vaccinated than those without a degree. Nearly 25% of all adults without a college degree fall into the vaccine hesitancy group. People in the “wait and see” group tend to be the young and people of color.  Reasons for Vaccine Hesitancy: To overcome vaccine hesitancy it is important to understand the root causes. The predominate cause is misinformation, but here is a partial list of other reasons.
Overcoming Vaccine Hesitancy
 Here are some other messaging points put together by Sherita Hill Golden, MD, Professor of Medicine at Johns Hopkins, to assist in overcoming vaccine misinformation:



Consequences of Not Getting Vaccinated 

 Getting a COVID-19 vaccine is a very personal choice, and although I believe that most adults should get vaccinated, it should not be forced upon them. There are some very legitimate reasons for some people not to get vaccinated, such as deeply held religious beliefs and some underlying medical conditions. For the benefit of the community, the country and the world, all people eligible to receive the vaccine should, for the common good.  There was a strong consistent message when the polio vaccine was introduced in the 1950s. It gained widespread acceptance under the banner “we’re all in this together”. Will this message resonate in our polarized world? Let’s hope and pray that it does.
Update July 13,2021: The pandemic is far from over, but you wouldn’t know it by walking down the streets of most American cities. The world recently surpassed the grim milestone of 4,000,000 deaths due to COVID-19. This was the official death toll, but the actual death toll is certainly much higher. Approximately 25% of the world’s adult population has received at least one shot of COVID-19 vaccine, mostly in the rich countries. Less than 1% of the adults in low- income countries (Africa, Asia, South America, Central America) have received a single shot of the vaccine. On June 15th the U.S. surpassed 600,000 deaths due to COVID-19, and the death rate continues to climb, mainly among those who have been unvaccinated. President Biden missed his July 4th goal of getting 70% of eligible adults vaccinated with at least one shot. As of this writing just under 68% of adults have received at least one shot. COVID-19 cases have come down significantly in the U.S. over the past few months due to the highly effective vaccines. As a result, most areas of the country have dropped all COVID-19 related restrictions. Mask mandates, social gathering restrictions, and indoor business restrictions have disappeared, and domestic travel has returned with a vengeance. But this rosy picture hides vast geographic disparities which show a significant rise in hospitalization rates and deaths due to COVID-19 in regions with low vaccination rates. Rural areas, which tend to be conservative, have seen a recent rise in COVID-19 cases. Low vaccination rates make these populations vulnerable to the highly contagious Delta variant. Arkansas and Missouri are seeing the worst outbreaks, followed by Florida, Nevada, Wyoming, and Utah. But unvaccinated people are driving increases in COVID-19 cases even in areas with high vaccination rates. This corresponds with the lowering (or elimination) of COVID restrictions and the emergence of the Delta variant. I live in a county north of San Francisco, where 68% of eligible people are fully vaccinated and another 8% are partially vaccinated. But there has been a troubling uptick in COVID-19 cases and hospitalizations, even before the full effects of 4th of July gatherings are felt. The vast majority of the hospitalized COVID-19 patients are unvaccinated. Contact tracing has shown that most of the current COVID-19 cases in my county are being fueled by social gatherings and leisure time activities, with the highest rates in the 18-32 age group. Vaccine hesitancy continues to align significantly with party affiliation. According to a recent Washington Post-ABC News poll, 6% of Democrats said they are not likely to get vaccinated, compared with 47% of Republicans, including 38% of Republicans who said they definitely will not get the vaccine https://www.washingtonpost.com/politics/post-abc-poll-biden/2021/07/03/54e95b6e-db43-11eb-8fb8-aea56b785b00_story.html. First detected in India, the Delta variant is estimated to be 60% more transmissible than earlier variants. The Delta variant has rapidly spread around the globe and is currently driving COVID-19 outbreaks in African, Asia, Australia and South America. The CDC has determined that the Delta variant is now dominant in the U.S. and is spreading rapidly in unvaccinated populations. Researchers in France, Israel and Britain have shown that a single dose of the Pfizer or AstraZeneca vaccine is largely ineffective against the Delta variant. Therefore, delaying the second shot in order to vaccinate more people is no longer an effective option. New variants, like the Lambda variant spreading rapidly in South America, provide more reason to quicken the pace of vaccination around the world. The unvaccinated population provides a breeding ground for new variants, and short of shutting down the world, vaccines are our only real defense. Pfizer made news last week by announcing that it would seek FDA approval for a COVID-19 booster vaccine. The CDC and NIH strongly rejected the need for vaccine boosters at this time, refuting the claims made by Pfizer. But many in the scientific community acknowledge that it is not a matter of if, but when booster shots will be needed. Preliminary research out of Israel suggests that the Pfizer vaccine is less effective against the Delta variant and there is a decline in antibody levels against the virus over time. I think that we should be prepared for the eventuality of booster shots, but we need to think through the ethical issues involved. Is it ethical to provide booster shots to fully vaccinated people in wealthy countries when the vast majority of people in poorer countries remain unvaccinated? Israel plans to offer booster shots of the Pfizer vaccine to adults with weakened immune systems, and Britain has announced plans to provide booster shots to its vulnerable populations and front-line workers. It makes sense to protect our most vulnerable, but it seems premature to do so when there is a limited supply of vaccines. The FDA warned this week that the Johnson & Johnson COVID-19 vaccine can lead to an increased risk of Guillain-Barré syndrome, a rare neurological condition. The incidence is very rare, and the benefits of this highly effective vaccine outweigh the risks. But I fear that this warning from the FDA will further diminish the acceptance of this much needed vaccine. The vast majority of hospitalizations and deaths due to COVID-19 are occurring in unvaccinated people. The evidence is overwhelming. Unvaccinated people pose a risk to themselves and to vulnerable populations who have been vaccinated. No vaccine is 100% effective and breakthrough infections do occur. The incidence of COVID-19 is eleven times higher in unvaccinated people than vaccinated ones. If that isn’t an incentive to get vaccinated, I don’t know what is. Encourage everyone you know to get vaccinated. Regarding the use of face masks, do like I do, don’t leave home without one. If you enjoy reading this type of commentary please subscribe to my blog and tell a friend. You will receive an email notification when new blogs are posted. The email will come from the site’s email: armchairamerican1776 @gmail.com. Thanks, Armchair American  It has been over two months since my last BLOG on COVID-19 vaccines. Since that time millions of people in several different countries have been vaccinated, new vaccines have been approved for use, and new virus variants have emerged. This blog is about the latest developments on the COVID-19 vaccine front.  Johnson & Johnson (J&J) Vaccine: The J&J vaccine was given Emergency Use Authorization by the F.D.A. on February 27, 2021. According to Johnson & Johnson’s press release, the vaccine was 72% effective at preventing moderate to severe COVID-19 infections in the U.S. (https://www.jnj.com/johnson-johnson-announces-single-shot-janssen-covid-19-vaccine-candidate-met-primary-endpoints-in-interim-analysis-of-its-phase-3-ensemble-trial). What this means is the vaccine prevented all illness, including mild symptoms, in 72% of the recipients of the vaccine. This may sound disappointing in comparison to the 94-95% efficacy of the Pfizer-BioNTech and Moderna vaccines, but it was highly effective at limiting serious disease. J&J’s vaccine was 85% effective overall at preventing serious illness across all regions that it studied (U.S., Argentina, Brazil, Chile, Columbia, Mexico, Peru, and South Africa). More importantly, the vaccine demonstrated complete protection against COVID-19 related hospitalizations and deaths, the true benchmarks of the success of this vaccine. The vaccine had an overall efficacy rate of 64% against the more virulent South African strain, but an 82% rate against serious illness. It is important to note that the J&J trials were conducted when more variants were circulating in the population than when the Pfizer-BioNTech and Moderna trials were being conducted. This could account for the reduced efficacy being reported in the U.S. and elsewhere. Here are the key attributes of this new vaccine:
The J&J vaccine is a breakthrough. It doesn’t need sophisticated freezers for transport and storage, making it accessible to remote and underserved areas, as well as in second and third world countries. The fact that it is effective after a single dose makes it a great choice when scheduling a second shot is problematic, such as in homeless populations, the homebound, migrant farm workers, and hard to reach populations around the world. If I was the vaccine czar, the J&J vaccine would be reserved for these vulnerable populations.  Pfizer-BioNTech Vaccine: On February 12, 2021, Pfizer-BioNTech announced that the U.S. government had exercised its option to purchase an additional 100 million doses of their vaccine. This brings the total number of doses to be supplied to the U.S. to 300 million, enough for 150 million people. Here are some recent developments:
 Moderna Vaccine: On February 11, 2021 Moderna announced that the U.S. government had agreed to purchase an additional 100 million doses of its vaccine. This brings the total confirmed order commitment to 300 million doses, enough to fully vaccinate 150 million Americans. Moderna is on track to deliver the first 100 million doses in the first quarter of 2021, the next 100 million in the second quarter, and the new order of 100 million doses by the end of July 2021. Even without any new vaccines becoming available, the U.S. now has enough contracted vaccines to cover all of its eligible citizens, and then some. Here are some recent developments:
 AstraZeneca/University of Oxford Vaccine: This vaccine was first approved for emergency use in the United Kingdom on December 30, 2020 for individuals 18 years of age and older. The vaccine requires a two-dose regimen, with an interval of between four and twelve weeks between doses. There has been some debate about the actual efficacy of the vaccine, with ranges from 62-82%. But clinical trials in the United Kingdom have shown the vaccine to be safe and highly effective at reducing hospitalizations and deaths. Because of the confusion over some of the reported data, the U.S. is conducting a trial of its own. Approval in the U.S. may still be a few months away. The vaccine can be transported and stored at normal refrigeration temperatures (36-46°F) for at least six months, making it a good candidate for use in 2nd and 3rd world countries. Here are some recent developments:
 Novavax: On January 28, 2021, Novavax announced that its vaccine demonstrated 89% efficacy in a Phase 3 clinical trial conducted in the United Kingdom (https://ir.novavax.com/news-releases/news-release-details/novavax-covid-19-vaccine-demonstrates-893-efficacy-uk-phase-3). Preliminary studies suggest that it is very effective at preventing severe disease from the South African strain of COVID-19. Phase 3 clinical trials are underway in Mexico and the U.S. and should be concluded by the end of March. The vaccine requires two-doses, but doesn’t require the strict storage requirements of the Pfizer-BioNTech or Moderna vaccines. In September Novavax entered into an agreement with a major Indian vaccine manufacturer that could produce up to 2 billion doses per year. The U.S. has an agreement to purchase up to 110 million doses, with most of the remaining doses going to the COVAX Alliance. Look for this vaccine to be approved for use in the second half of 2021. There are currently 71 COVID-19 vaccines in clinical trials on humans, 20 of these have reached large scale Phase 3 trials around the world. In addition to the five vaccines that I detailed above, China has two vaccines it has approved for use, Russia has one vaccine, as does India.  Virus Variants: The longer the novel coronavirus circulates, the more people that become infected, giving the virus opportunities to mutate into more dangerous variants. Any new variant has the potential of being more contagious, result in more severe illness, and be resistant to currently available vaccines. This is why it is so important to speed up the rate of vaccinations and to continue safe practices, until herd immunity is reached. Widespread testing for COVID-19 is very important to monitor the development and spread of new variants. Here are some of the new variants which have recently been identified:
 Vaccine Equity: As of this writing approximately 240 million doses of vaccine have been administered around the world (https://www.cnn.com/interactive/2021/health/global-covid-vaccinations/). According to the United Nations, ten countries administered 75% of all vaccines, and 130 countries have yet to receive a single dose. The COVAX Alliance, led by the World Health Organization, is working with rich countries to provide vaccines to poor ones. But it is off to a slow start. COVAX delivered its first shipment of 600,000 doses of the AstraZeneca vaccine to Ghana on February 24, 2021. Ghana is one of 190 countries which have signed up to receive vaccines through the alliance. The COVAX Alliance currently has agreements with AstraZeneca and Novavax for COVID-19 vaccines, but the numbers are far short of what is needed. It is important to remember that no one is immune from COVID-19 until we are all immune.  What We Still Don’t Know: We are a year into this pandemic, vaccines have only been available in limited supply for about two months, and there are a lot of unanswered questions. Once vaccinated, are people still able to spread the virus? Once vaccinated, how long will immunity last? If you had COVID-19, how long does immunity last? When will herd immunity be reached? Well, this is the real question, and we all need to be patient.
As of today, about 14.6% of the U.S. population has received at least one shot of vaccine, and a tiny fraction of the world’s population has been vaccinated. It is important to get vaccinated when it is your turn, but it is also important to continue to wear your face mask, practice social distancing and continue using good hygiene. We can't afford to let our guard down now that there is light at the end of the tunnel. We won't know that herd immunity has been reached until new cases of COVID-19 infections are rare. The speed with which the various COVID-19 vaccines have been developed and gotten into peoples’ arms is truly remarkable. All of the vaccines currently available in the U.S. are highly effective at minimizing serious illness and death. Coronaviruses have been circulating within the human population for centuries, and the coronavirus that causes COVID-19 will be with us for a long time. The sooner that the majority of the world’s population becomes vaccinated, the sooner the pandemic will be over, and the quicker we will all return to a semblance of “normalcy”. If you enjoy reading this type of commentary please subscribe to my blog and tell a friend. You will receive an email notification when new blogs are posted. The email will come from the site’s email: armchairamerican1776 @gmail.com. Thanks, Armchair American  Joy to the world, the vaccines have come. Let earth begin to heal. Let's thank those who delivered them; let every arm prepare for one; and heaven and nature sing, and heaven and nature sing, and heaven and heaven, and nature sing. Is this a Christmas miracle? Let’s not get ahead of ourselves. This is still 2020 after all, and we have a long road ahead. The two COVID-19 vaccines currently in limited distribution were developed in record time, but the development of the technologies behind the vaccines took decades. Let’s look at the two vaccines currently being distributed and what to expect in the coming months.  Operation Warp Speed (OWS): A public-private partnership initiated by the U.S. government to facilitate and accelerate the development, manufacturing, and distribution of COVID-19 vaccines, therapeutics, and diagnostics (https://www.hhs.gov/coronavirus/explaining-operation-warp-speed/index.html). This is an interagency program spearheaded by the Department of Health and Human Services. The main goal of this program is to produce and deliver 300 million doses of safe and effective vaccines, with the initial doses available by 2021. So far so good. The Chief Operating Officer of the program is General Gustave Perna, and the Chief Scientific Advisor is Moncef Slaoui.  In August, OWS chose six companies to receive funding in order to expedite development and manufacture of COVID-19 vaccines. These companies are Johnson & Johnson, Moderna, Astra Zeneca/University of Oxford, Novavax, Merck, and Sanofi/GlaxoSmith Kline. Pfizer/BioNTech did not receive any direct funding from OWS, but has agreed to supply vaccines. Pfizer/BioNTech COVID-19 Vaccine: This vaccine was given Emergency Use Authorization (EUA) by the FDA on December 11, 2020. This is not the same as a full FDA approval, but it allows the vaccine to be used because there is sufficient evidence to show that its potential benefits outweigh its risks. Nearly 3 million doses of vaccine were delivered over the last ten days to 636 sites across the U.S. An additional 3 million doses will be delivered over the next few weeks to complete the required two dose regimen. Twenty to thirty million doses will be delivered each month in the first quarter of 2021. The first vaccines began to be administered to frontline healthcare workers on December 14, 2020. The vaccine was developed in Germany by BioNTech using mRNA technology (https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/mrna.html). BioNTech has partnered with Pfizer to help fund, manufacture, and distribute the vaccine. OWS has contracted with Pfizer to purchase 100 million doses of the vaccine for $1.95 billion. Pfizer will produce about 1.3 billion doses of the vaccine in 2021 to be distributed around the world. The U.S. government is currently negotiating with Pfizer for an additional 100 million doses of vaccine, but Pfizer lacks the required raw materials. The government is considering using the Defense Production Act to speed up production of the needed materials. In an interview with CNBC, Pfizer CEO Albert Bourla said he would welcome the U.S. government’s help in procuring needed materials in order to increase production of the vaccine. This just in: Today (12/23), Pfizer and BioNTech have signed a $2 billion agreement with the U.S. government for the purchase of an additional 100 million doses of COVID-19 vaccine. At least 70 million doses will be delivered by June 30, 2020, and the remaining 30 millions doses will be delivered no later than July 31, 2020. What You Need to Know About the Pfizer Vaccine:
You can find more information on the Emergency Use Authorization of the Pfizer Covid-19 vaccine at: (https://www.fda.gov/media/144414/download). Moderna COVID-19 Vaccine: This vaccine was given Emergency Use Authorization by the FDA on December 18, 2020. The FDA stated that its analysis “supported a favorable profile”, and confirmed Moderna’s earlier assessment that its vaccine was 94.1% effective. Administration of this vaccine began on December 21, 2020. The Moderna vaccine is roughly equivalent to the Pfizer vaccine, both of which use synthetic messenger RNA technology. Moderna is a small biotech company based in Cambridge, Massachusetts, and the vaccine is the first product it has brought to market. Moderna will rely on contract manufacturers, such as Catalent Biologics in Indiana, to package and distribute their product. They plan to produce 500 million doses in 2021. Unlike Pfizer, Moderna has worked closely with Operation Warp Speed. The vaccine was developed in partnership with the National Institute of Allergy and Infectious Diseases, under-written by the government. Last summer the government signed a contract to purchase 100 million doses of the vaccine to be delivered in the first quarter of 2021. Earlier this month the government signed another agreement to purchase an additional 100 million doses to be delivered by the end of the 2nd quarter. This brings the government’s investment in the Moderna vaccine to $4.1 billion. What You Need to Know About the Moderna Vaccine:
You can find more information on the Emergency Use Authorization of the Moderna Covid-19 vaccine at: (https://www.modernatx.com/covid19vaccine-eua/). Other COVID-19 Vaccines on the Horizon in the U.S.:


 Vaccine Distribution: Operation Warp Speed is coordinating distribution of all vaccines. It is allocating vaccines according to each state’s population. The CDC has established guidelines to aid the states in prioritizing the limited supply of vaccines. The individual states have the final say on how the vaccines will be distributed, but most states will follow the CDC guidelines. The highest priority (Phase 1a) will be frontline healthcare workers and older people and staff in residential care homes. The CDC just released new guidelines for people in the next priority group (Phase 1b). This group includes people 75 and older, and frontline workers in “essential” jobs. These essential workers include teachers, emergency workers, and people who work in grocery stores, prisons, food processing plants, and public transportation. It will probably take most of the 1st quarter of 2021 to vaccinate this group of people, assuming no supply disruptions. The next group (Phase 1c) will be people aged 65-74, and younger people with high- risk health conditions. Even if we wanted to vaccinate everyone sooner, the supply just isn’t there. Phase I alone will use most of the vaccines currently contracted for through Operation Warp Speed. The country will need at least one more approved vaccine to get all of the general public vaccinated by the end of the summer. The National Governors Association and Duke University have developed a website to help navigate the vaccine distribution across the country. For your state’s specific plan follow this link: (https://healthpolicy.duke.edu/news/covid-19-vaccination-plans-state). The CDC has established the “Pharmacy Partnership for Long-Term Care” to offer onsite COVID-19 vaccination services for residents and staff of nursing homes and assisted living facilities. The participating pharmacies include CVS, Walgreens, and Managed Health Care Associates.  How Much Will the Vaccine Cost?: The federal government (tax payers) is paying for the vaccine. Healthcare providers may charge an administration fee, but in most cases this will be covered by medical insurance.  Will Vaccination be Mandatory?: At this time vaccination is voluntary. It would be legally questionable to mandate vaccination with a product that has not received full FDA approval. But it is likely that there will be travel restrictions put in place requiring people to be vaccinated before flying or entering certain foreign countries. Will the Vaccines be Effective Against New Virus Variants: According to HHS officials and reports from Pfizer and Moderna, there is a high level of confidence that existing vaccines will be effective against new COVID variants, such as the one in the United Kingdom(UK). Moderna and Pfizer will conduct tests on the UK variant in the coming weeks to make certain that their vaccines are effective. Challenges Remain:

 Vigilance and Patience: It will take most of 2021 to get the majority of the eligible people in the U.S. vaccinated against COVID-19. This is a massive effort and hiccups are bound to happen. We all just need to be patient. While we wait for herd immunity to be achieved, which could be many months to years away, we need to continue to protect ourselves, our families, and communities against the virus. This means that mask wearing, social distancing, and hand sanitation are as important as ever. Even after people become vaccinated, they may still shed the virus, so we must remain vigilant. New information about the coronavirus, COVID-19, and vaccines is coming out daily, so stay informed. The vaccines currently available, and those in development, give us hope for 2021. The efforts behind these vaccines demonstrate what can be accomplished when thousands of people in the public and private sectors come together in common cause for the betterment of humanity. The true Christmas miracle would be if this becomes a trend, and people come together to solve intractable problems like homelessness, poverty, hunger, racial injustice, the failed healthcare system, etc., etc., etc. One can only wish; and here’s wishing you a Merry Christmas.  If you enjoy reading this type of commentary please subscribe to my blog and tell a friend. You will receive an email notification when new blogs are posted. The email will come from the site’s email: armchairamerican1776 @gmail.com.
Thanks, Armchair American  On November 25, 2020, in a 5-4 ruling, the U.S. Supreme Court sided with religious organizations in a case over COVID-19 restrictions put in place by New York Governor Andrew Cuomo. The recent appointment of Justice Amy Coney Barrett has given the court a conservative majority, so the ruling should not be surprising. Is this ruling a shadow of things to come for the high court or just a one-off event? Let’s take a closer look.  I am not a lawyer. The extent of my legal training is a few graduate level courses in business and tax law. When I am confronted with a constitutional issue that I am not familiar with I first consult the relevant articles in the U.S. Constitution. Then I attempt to determine the intention of the writers of the Constitution by reviewing the Federalist Papers, and any other pertinent writings. Finally, I see if there have been any similar cases ruled on by the Supreme Court which may have established a precedent for the issue under review. Fortunately, I have already researched and addressed the constitutionality of pandemic restrictions in my previous blog "are-pandemic-restrictions-violating-your-first-amendment-rights.html". From the previous blog on this topic we know that states have broad powers to restrict individual liberties in the name of public health. In issues of medical and scientific uncertainties, state health officials should not be subject to second-guessing by an unelected federal judiciary which lacks the background, competence, and expertise to assess public health matters. Restraints may be placed on constitutional rights by the state for the common good. However, the restrictions have to be applied without preference to content or viewpoint. For example, if officials restrict indoor religious gatherings to 50 people, they must restrict all indoor gatherings to 50 people. This is where I think the State of New York crossed over the line. The state singled out houses of worship and imposed harsh restrictions on indoor religious gatherings. Let’s take a look at the case.  Roman Catholic Diocese of Brooklyn, New York v. Andrew M. Cuomo, Governor of New York : www.supremecourt.gov/opinions/20pdf/20a87_4g15.pdf The Catholic Diocese of Brooklyn, along with Agudath Israel of America sought to overturn an Executive Order issued by Governor Cuomo which imposed restrictions on attendance at indoor religious services taking place in “red” or “orange” zones. In red zones, no more than ten people could attend each religious service, and in orange zones, attendance was limited to twenty-five. The religious groups claimed that this was in violation of the Free Exercise (of religion) Clause of the First Amendment. They argued that the regulations treated houses of worship much more harshly than comparable secular facilities. Five of the nine justices agreed, writing that “…the regulations cannot be viewed as neutral because they single out houses of worship for especially harsh treatment”. As an example, in an orange zone attendance at houses of worship is limited to twenty-five people, even though non-essential businesses may decide for themselves how many people to admit. It should be noted that before this case was decided, Governor Cuomo reclassified the areas in question from orange to yellow, allowing for religious services to take place at 50% of their maximum capacity. However, the Court went forward with the case because the Governor could enact more restrictive classifications at any time.  Implications of the Ruling: The case’s immediate impact is narrow, setting aside two specific restrictions on attendance at houses of worship in New York. The ruling did not overturn all pandemic restrictions at houses of worship, such as mask wearing and social distancing mandates. I don’t think that this case sheds any additional light on how Justice Amy Coney Barrett will rule in future cases. She did vote with the conservative majority, but did not issue her own opinion. The most telling opinion was written by Trump appointee Neil Gorsuch. He wrote, “Government is not free to disregard the First Amendment in times of crisis”. He went on to write that the court precedent that Chief Justice Roberts cited in a related California case, “…hardly supports cutting the Constitution loose during a pandemic”. You may read the full text of the case and accompanying opinions at the link cited above.  Earlier in the year the Supreme Court upheld indoor religious service restrictions in California and Nevada: (https://www.supremecourt.gov/opinions/19pdf/19a1044_pok0.pdf). These restrictions were not as severe as the ones in New York, and applied equally to religious and secular organizations. The new conservative court may have a different view. The New York case will certainly embolden religious groups, and we will soon see challenges to California’s restrictions on indoor religious gatherings. Just this Thursday the AP reported that the Supreme Court ordered a lower federal court to reexamine California restrictions on indoor religious services in light of the recent ruling in New York. With COVID-19 cases surging in California, it is uncertain if the Governor’s restrictions will stand. What does seem certain is that Chief Justice Roberts will have a challenging time holding sway over the five conservative justices, and his position as the swing voter on the Court has been neutered.  I agree with the Supreme Court’s ruling overturning New York’s attendance restrictions on religious gatherings. These restrictions specifically targeted houses of worship in violation of their First Amendment rights. New York classified such businesses as liquor stores, bicycle repair shops, hardware stores, and acupuncturists as “essential”, and therefore not subject to capacity restrictions. This seems arbitrary. Does it make any kind of sense to restrict a 1000 seat church to ten or even twenty-five attendees when it is legal to cram 200 people into the passenger cabin of a jetliner for a six-hour transcontinental flight? Not to get sidetracked, but most airline travel today is nonessential, and a passenger may take off their mask to eat or drink. Sounds like an indoor restaurant to me, but restaurants are no longer allowed to offer indoor dining. My point is, that it is a slippery slope when we allow public officials to pick winners and losers. When that happens, we have a lot more to lose than just our religious freedoms. As for the new conservative court, governors have been warned that they better carefully consider any restrictions that interfere with the free exercise of religion, even during a pandemic.  February 23, 2021 Update: On February 5, 2021 the Supreme Court ruled that California’s ban on indoor church services violated the free exercise of religion guaranteed by the First Amendment. But the Court kept in place prohibitions on singing and chanting, and allowed the state to limit indoor services to 25% of the building’s capacity. This is not surprising in light of a similar ruling in New York last November.
The decision was 6-3, with the majority arguing that California had singled out places of worship for unfair treatment. This is hard to argue against since some religious buildings are the size of whole city blocks, and restricting any attendance in such buildings seems arbitrary and not grounded in science. The Court’s three liberal decenters stuck to the belief that the Court should not overrule the public health experts during an ongoing pandemic. If you enjoy reading this type of commentary please subscribe to my blog and tell a friend. You will receive an email notification when new blogs are posted. The email will come from the site’s email: armchairamerican1776 American @gmail.com. Thanks, Armchair American Public Health Should be Above Politics. Was a Line Crossed in Favor of Black Lives Matter Protests?8/15/2020  As was established in the last blog post, public health authorities have broad powers under the constitution to restrict individual liberty to combat a health crisis. However, these restrictions must be applied fairly, without prejudice to content or viewpoint. Black Lives Matter protests have been taking place across the country for over two months, in apparent violation of social distancing and public gathering restrictions. Have the public health authorities crossed the “neutral” line? In the wake of the George Floyd killing by Minneapolis police, demonstrations against police brutality have erupted across the country. Black Lives Matter protests took place in cities large and small. This became real to me when protests shut down Highway 101 running through the middle of Santa Rosa, on the evening of June 5. Unable to make it home on the 101, I took an alternative route through the city’s downtown. I soon ran into the middle of a group of people marching through the city chanting “Black Lives Matter”. The protest was peaceful and I never felt threatened. Several nights of protests followed in the downtown area. Some looting and vandalism did occur late at night, long after most of the peaceful protestors had left. All this got me thinking “what about the public health orders put in place to stop the spread of the coronavirus”? There were orders in place to restrict outdoor gatherings to 100 attendees, as well as social distancing and face covering requirements. I reached out to city and county officials for answers, but never received any. My city was not alone. Major protests and marches were taking place in Milwaukee, New York, Washington DC, Seattle, Denver, Portland, San Francisco, Los Angeles, Philadelphia, and in hundreds of cities across our country. COVID-19 was no longer public health enemy number one. It had been replaced by police brutality and systemic racism.  Many public officials took part in the protests, including the mayors of Minneapolis and Washington DC, chiefs of police, including the one in my city, and the Governor of New Jersey Phil Murphy. But most of these protests were taking place in cities which restricted public gatherings to 50-100 people. Social distancing and facial covering mandates were in place as well. This is why shouts of “liberal hypocrisy” started to be heard (https://www.politico.com/news/2020/06/06/conservatives-charge-liberals-with-social-distancing-hypocrisy-304435). Opponents of New Jersey Governor Murphy claimed that he was violating his own executive order by picking winners and losers by blurring the line between protests “worthy of participation and those deserving prosecution”(https://www.fox5ny.com/news/nj-governor-questioned-about-attending-rallies-during-stay-at-home-order  Apparently not all protests are created equal. Conservatives have pointed out that lockdown protests during April and May were prohibited by public health officials because they violated social distancing and public gathering restrictions. But the protests against police brutality, which began in late May, appear to be condoned by the public health community. Even though these recent protests have occurred as many cities began lifting stay-at-home restrictions, and many of the protestors wore face coverings, there is much evidence in support of the conservative view. A national group of 1,288 health professionals signed the “Open letter advocating for an anti-racist public health response to demonstrations against systemic injustice occurring during the COVID-19 pandemic”. The open letter (https://drive.google.com/file/d/1Jyfn4Wd2i6bRi12ePghMHtX3ys1b7K1A/view) states “white supremacy is a lethal public health issue”, and “in addressing demonstrations against white supremacy, our first statement must be one of unwavering support for those who would dismantle, support, or reform racist institutions”. The open letter further states that “as public health advocates, we do not condemn these gatherings as risky for COVID-19 transmission. We support them as vital to the national public health and to the threatened health specifically of Black people in the United States”. The open letter also spells out why the Black Lives Matter protests are different than the earlier protests against stay-at-home orders.  The American Public Health Association declared systemic racism a public health crisis at the beginning of June. Soon after, Colorado, Wisconsin and Michigan, along with cities in several other states, have declared systemic racism to be a public health emergency or crisis (https://www.apha.org/topics-and-issues/health-equity/racism-and-health/racism-declarations). One of the key justifications for these declarations is that COVID-19 has affected communities of color at a disproportionate rate. I think that the public health community is justified in shining a light on systemic racism. It has clearly led to many inequities in our society, particularly in areas of housing, education and health outcomes. According to recent polls, most Americans support the views of the Black Lives Matter protests (https://news.gallup.com/poll/316106/two-three-americans-support-racial-justice-protests.aspx).
But, is there legal justification to favor one form of protest over another? Probably not. But that’s for the courts to decide. Even though public health officials have broad constitutional powers during health emergencies, there are limits. Consider this: people are shot and killed on a daily basis in several of our major cities, namely Detroit and Chicago. Why not just declare public health emergencies in these cities and ban guns outright? Gun violence is clearly a public health crisis, and public health officials have broad authority under such conditions. Unfortunately, this won’t happen. The gun culture in American is as deeply rooted as is systemic racism, and constitutionalists wouldn’t allow it. Gun violence is another epidemic that needs to be tackled, but that’s an issue for another day. Mass gatherings of people, regardless of how righteous the cause, increases the risk of spreading COVID-19. As we have seen, many people in public health feel that getting the message out about systemic racism is worth the risk. The early restrictions put in place to stop the spread of COVID-19 were backed up by science. It appears that by allowing Black Lives Matter protests to continue, science has taken a backseat to political considerations. I’m afraid that many public health officials have undermined their credibility by messaging that certain behaviors can be sanctioned if the cause is just. Public health should be above politics. You may feel that public health officials are justified in favoring the Black Lives Matter protests. That’s for you, and perhaps the courts to decide. But what is clear, is that the partisan divide over the coronavirus response has widened. Messaging about actions to defeat the virus has become more confused, and trust in the Public Health System may have been diminished. This certainly doesn’t help at a time when a united, clear, and coherent plan to deal with the pandemic is needed. The COVID-19 pandemic is far from over. I just hope that the public continues to listen to and heed the advice of our public health experts. If you enjoy reading this type of commentary please subscribe to my blog and tell a friend. You will receive an email notification when new blogs are posted. The email will come from the site’s email: [email protected]. Thanks, Armchair American  The First Amendment to the U.S. Constitution guarantees basic rights or freedoms to the people of the United States. They are the freedom of religion, freedom of speech, freedom of the press, the right to peaceably assemble, and the right to petition the Government. In recent months Public Health Departments, in conjuction with state and local officials, have among other measures, placed restrictions on public gatherings and religious gatherings. Doesn’t that violate our constitutionally guaranteed rights? The short answer is, not always. Let’s take a look. There are many cases winding their way through the courts, challenging governors in various states who have put restrictions in place to stop the spread of COVID-19. Most of the cases challenge restrictions placed on houses of worship in violation of the First Amendment’s freedom of religion clause. The other significant group of cases challenge restrictions limiting peaceful protests and other gatherings, in violation of the First Amendment’s right to peaceably assemble. In order to determine the constitutionality of pandemic restrictions placed by the various states, we have to turn to the Supreme Court.  The first coronavirus related case to be ruled on by the Supreme Court was South Bay United Pentecostal Church V. Newson, No. 19A1044 (May 29, 2020). The church had filed a lawsuit against California Governor Gavin Newsom after he put in place an Executive Order limiting attendance at places of worship to 25% of building capacity or a maximum of 100 attendees. The church claimed that this violated their First Amendment rights. The Supreme Court rejected the church’s claim, and upheld Governor Newsom’s right to place restrictions on in-person religious services in an attempt to control the spread of the coronavirus. But how can that be? It is a clear case of government restricting the free exercise of religion. Here’s what Chief Justice Roberts had to say in his majority opinion: “The Governor of California’s Executive Order aims to limit the spread of COVID-19, a novel severe acute respiratory illness that has killed thousands of people in California and more than 100,000 nationwide. At this time, there is no known cure, no effective treatment, and no vaccine. Because people may be infected but asymptomatic, they may unwittingly infect others. The Order places temporary numerical restrictions on public gatherings to address this extraordinary health crisis”. The opinion further states that “…those restrictions appear consistent with the Free Exercise Clause of the First Amendment. Similar or more severe restrictions apply to comparable secular gatherings, including lectures, concerts, movie showings, spectator sports, and theatrical performances, where large groups of people gather in close proximity for extended periods of time”. The California order was neutral regarding its treatment of all in-door gatherings, religious and secular, and therefore lawful. For a full reading of the Supreme Court opinion go to: https://www.supremecourt.gov/opinions/19pdf/19a1044_pok0.pdf . This case has wider implications over the debate regarding coronavirus restrictions. According to the Roberts’ opinion, “Our Constitution principally entrusts the safety and health of the people to the politically accountable officials of the States to guard and protect.” Roberts is citing here a precedent established by Jacobson v. Massachusetts, 197 U.S. 11, 38 (1905). This case upheld the authority of states to enforce compulsory vaccination laws because the regulation in question was “necessary in order to protect the public health and secure the public safety”. The decision further explained that individual liberty is not absolute and is subject to the police power of the state. “There are manifold restraints to which every person is necessarily subject for the common good. On any other basis organized society could not exist with safety to its members. Society based on the rule that each one is a law unto himself would soon be confronted with disorder and anarchy”: https://tile.loc.gov/storage-services/service/ll/usrep/usrep197/usrep197011/usrep197011.pdf . Roberts opinion continues: “When those officials undertake to act in areas fraught with medical and scientific uncertainties, their latitude must be especially broad. Where those broad limits are not exceeded, they should not be subject to second-guessing by an unelected federal judiciary which lacks the background, competence, and expertise to assess public health and is not accountable to the people.” The bottom line is, the courts are going to defer to elected officials in the states to determine how best to protect the health and safety of its citizens during the pandemic.  According to Christopher Dunn of the New York Civil Liberties Union, Jacobson V. Massachusetts will be the case that frames all litigation around coronavirus-based restrictions on public gatherings. What happens when the government starts rolling out a coronavirus vaccine later this year or next year? Can the government force me to take it? In a word, yes. Jacobson v. Massachusetts specifically states that “It is within the police power of a State to enact a compulsory vaccination law, and it is for the legislature, and not for the courts, to determine….”. There are specific exemptions to vaccination laws which I will address in a future blog post.
The Supreme Court has also rejected lawsuits from churches in Illinois and Nevada looking to strike down coronavirus restrictions. Does this mean that all lawsuits challenging coronavirus restrictions are doomed to fail? Not necessarily. The restrictions have to be applied without preference to content or viewpoint. For example, if officials restrict in-door religious gatherings to 50 people, they must restrict all in-door gatherings to 50 people. It would be unconstitutional to allow a 100 person “Black Lives Matter” protest to take place and not a 100-person protest against coronavirus lockdowns. New York ran afoul of the content neutral requirement when it put into place bans on non-essential gatherings of individuals of any size for any reason, and then modified it. The modification allowed for gatherings of ten or fewer people for religious services, or for Memorial Day celebrations. This clearly favored two types of gatherings based upon the content of expression, and was therefore unconstitutional. New York was sued and subsequently modified its social gathering restrictions to allow groups of up to ten to gather for any lawful purpose or reason. Many of the “Black Lives Matter” protests seem to have violated restrictions on public gatherings. Did they receive preferential treatment? Perhaps. That will be the subject of the next blog post. I know that there was a lot of legalese to get through, but the issues presented are important. So, I have listed some of the important points to remember. Key Takeaways:
If you enjoy reading this type of commentary please subscribe to my blog and tell a friend. You will receive an email notification when new blogs are posted. The email will come from the site’s email: [email protected]. Thanks, Armchair American  A Universal Mask Mandate Could Make America Safe Again! In the first blog on face masks I examined the mixed messages surrounding the use of face masks by the general public, and the politicizing of the issue. In this blog I will review the issue of mandating the universal use of face masks, and the types of masks being used. No National Mask Mandate: Dr. Anthony Fauci, a key member of the president’s corona virus task force, has said many times that universal mask wearing is fundamental to stopping the spread of the coronavirus. But the president is against a national mask mandate, implying that it would deny Americans certain freedoms. Yes, we do enjoy many rights and freedoms in this country, but with rights come responsibilities. We are responsible for the safety of our communities and for each other. The president’s best chance of getting reelected is to step up, unite the country, and show true leadership in the fight against COVID-19. Turning the economy around wouldn’t hurt either, and here is where he has a real opportunity. A June 29, 2020 report by Goldman Sachs Research: https://www.goldmansachs.com/insights/pages/face-masks-and-gdp.html, shows evidence that a national mask mandate would reduce the need for broad lockdowns, slow the spread of the coronavirus, and increase GDP. You would think that this would be music to the president’s ears, particularly coming from a conservative institution like Goldman Sachs. But apparently not. A significant portion of individuals with COVID-19 lack symptoms and don’t know they are infected. This is why cloth face masks are most likely to reduce the spread of the virus when they are widely used in public settings. Research published by the “Proceedings of the National Academy of Sciences” examined COVID-19 hotspots in China, Italy and New York City. The research concluded that mandatory use of face coverings significantly reduced the number of infections in these areas, https://www.pnas.org/content/117/26/14857/tab-article-info . The researchers also conclude that “other mitigation measures, such as social distancing implemented in the U.S., are insufficient by themselves in protecting the public”. Since the president won’t put in place a national mandate for the use of face masks, it is up to the individual states to do so, and many have. 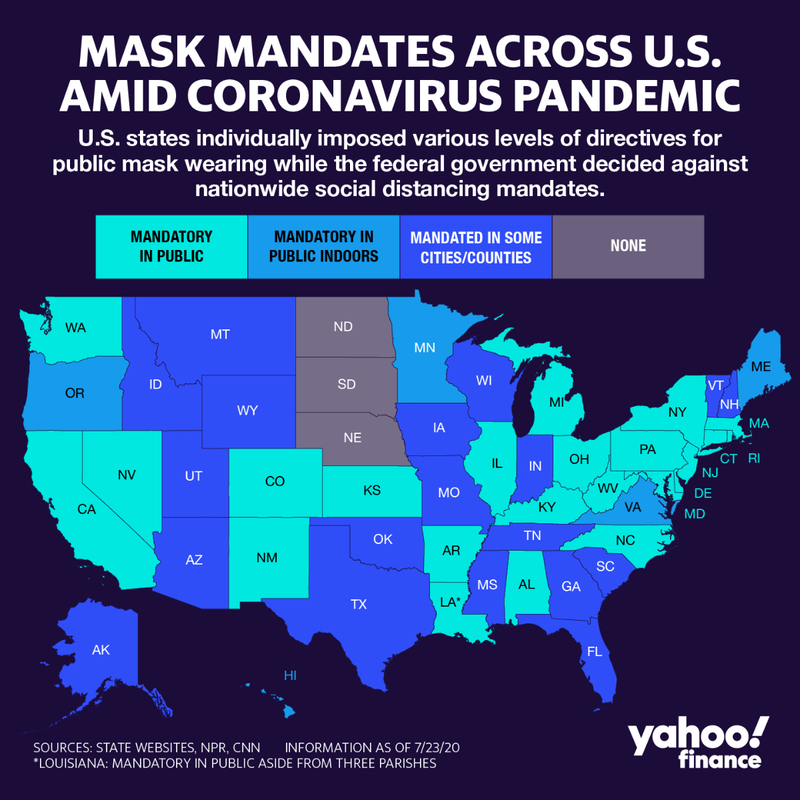 As of July 31, 2020, approximately 34 states and the District of Columbia have issued some form of mask mandate. There are several sites that are reporting on up to date mask mandates. CNN has a good site, with the specific mandates for each state: https://www.cnn.com/2020/06/19/us/states-face-mask-coronavirus-trnd/index.html . Another website that closely monitors mask requirements in individual states, as well as other countries is: https://masks4all.co/. Of note is the fact that the nation’s COVID-19 epicenter is now Florida, which does not have a statewide mask mandate. This exemplifies the haphazard and ad-hoc way in which the U.S. has approached the pandemic from the start, and it has been an unmitigated failure. We are over six months in, and rather than making progress, the country is sliding backwards. Mandating the universal wearing of face masks is much less painful, and much less costly, than shutting the economy down again. It is up to each citizen to do their part. National leadership on this issue is nowhere to be seen. Not all Face Masks are Created Equal: The coronavirus spreads mainly from person to person through respiratory droplets when an infected person coughs, sneezes, talks, or raises their voice. Medical masks, such as N95s, protect health care workers from catching coronavirus from infected people. Medical masks are regulated medical devices and are categorized as PPE (personal protective equipment). Medical masks should be reserved for health care workers. Cloth face coverings mainly prevent people who have COVID-19 from spreading the virus to others. Let’s take a closer look at these mask types.  N95 Respirator (N95s): This type of mask filters out 95% of airborne particles. It is designed to achieve a tight fit and is very efficient at filtering out airborne particles. The CDC does not recommend this type of mask for the general public due to critical shortages. N95s are reserved for health care workers and other medical first responders. They are designed not to be shared or reused, although some decontamination procedures do exist. The FDA has more information on N95s at this link: https://www.fda.gov/medical-devices/personal-protective-equipment-infection-control/n95-respirators-surgical-masks-and-face-masks.  Surgical Masks: These are loose fitting and create a physical barrier to prevent airborne contaminants from coming into contact with the nose and mouth. Like the N95, the CDC considers surgical masks to be critical PPE and are not recommended for use by the general public. Surgical masks come in various thicknesses, and are meant to be single use. Like the N95, surgical masks are regulated by the Federal Government.  Cloth Facial Coverings (Masks): These are also known as non-medical and fabric masks. They are not considered PPE and are not appropriate substitutes for N95s or surgical masks. Cloth masks are recommended by the CDC for use by the general public to help reduce the spread of the coronavirus. Cloth masks are now available at many online and brick and mortar stores. Many people (including my wife) make their own masks at home. The CDC website has a tutorial on making your own cloth face mask, as well as caring for them: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/how-to-make-cloth-face-covering.html. Cloth masks come in a variety of different fabrics (silk, polyester, cotton, felted wool), layering sequences, and shapes. Fabrics with higher thread counts offer better protection, and the more layers of cloth, the better. The WHO has reported on the filtration efficiency, and other considerations on a number of fabrics used in cloth masks: https://apps.who.int/iris/bitstream/handle/10665/332293/WHO-2019-nCov-IPC_Masks-2020.4-eng.pdf?sequence=1&isAllowed=y .  It is not required, but the addition of a filter between the layers of cloth adds an additional measure of protection. Some masks are made with a pocket so that filters may be added and removed. The best filters are made from polypropylene HEPA vacuum bags, or AC filters made from the same material. Another common filter is polyester interfacing, available at most fabric stores. Interfacing is a material used to strengthen and stabilize fabrics, and can be cut to size. Coffee filters and paper towels are sometimes used as well, but need to be changed before each use. According to a recent study, a minimum of two layers, and preferably three, are required to prevent the dispersal of droplets from an infected person. A summary of the study, along with video evidence, can be found at https://www.cnn.com/videos/app-health-section/2020/07/23/mask-test-study-wellness.cnn. The WHO also advises that fabric masks should consist of at least three layers of different material: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public/when-and-how-to-use-masks .
Other types of facial coverings that offer limited protection include bandanas, scarves and neck tubes or Buffs. The CDC recommends that cloth face masks be washed after each use. COVID-19 is caused by a novel (new) coronavirus, and our knowledge about it is increasing daily. We need to heed the advice of the scientific and medical communities, not politicians.  The biggest decision of my day is which mask to wear! Don’t leave home without one. If you want a good laugh, and who doesn’t these days, check out this great video from Randy Rainbow: https://www.youtube.com/watch?v=6kOesPt7iBY . If you enjoy reading this type of commentary please subscribe to my blog and tell a friend. You will receive an email notification when new blogs are posted. The email will come from the site’s email: [email protected]. Thanks, Armchair American  No President Allowed Without a Face Mask! I have received a lot of great feedback on the first blog post “Vote 2020”. I agree it was too long and should have been broken up into two or three separate posts. The next topic I will explore is the use of face masks during the coronavirus pandemic. I have split it into two posts for easier consumption. The evidence is clear, wearing facial coverings or face masks, helps to reduce the spread of coronavirus. I can’t find an epidemiologist, infectious disease specialist, or public health official who disagrees with this. I wear a face mask every time I leave the house, but many people don’t. Why is wearing a face mask still controversial, and why did a health crisis turn political? Here we are six months into the pandemic. Many states are experiencing increasing cases of COVID-19, and hospitals are nearing capacity in several major cities in Florida, Arizona, Texas and California. So how did we get here? We have received mixed messages on the coronavirus (SARS-CoV-2) since it was first detected in the U.S. in January. The virus was novel (new) and there was not much known about it. The coronavirus causes the Coronavirus Disease 2019 (COVID-19). During the early months of the pandemic, information coming out of the World Health Organization (WHO), the Centers for Disease Control and Prevention (CDC), and the Trump Administration, has caused a lot of confusion. This was particularly true regarding the use of face masks. We were first told not to wear face masks, now we are encouraged, but not always required to wear them. Here’s what some of these agencies and federal officials had to say: World Health Organization (WHO): The WHO first provided guidance on the use of face masks in a report entitled “Advice on the use of masks in the context of COVID-19: Interim guidance” dated January 29, 2020. This report stated that “There is currently no evidence that wearing a mask (whether medical or other types) by healthy persons in the wider community setting, including universal community masking, can prevent infection with respiratory viruses, including COVID-19”. It wasn’t until June 5, in an update to this guidance report, that the WHO tepidly sanctioned face mask use by the general public (https://apps.who.int/iris/bitstream/handle/10665/332293/WHO-2019-nCov-IPC_Masks-2020.4-eng.pdf?sequence=1&isAllowed=y). The report acknowledged that the WHO’s change in stance was due to observational evidence in several countries that face masks might help to reduce the spread of the COVID-19 virus. In this report the WHO also acknowledged that airborne transmission of the COVID-19 virus is possible. But the organization stuck to their belief that most transmission occurred from symptomatic people in close contact with others. We would latter learn that a significant amount of transmission is occuring from asymptomatic and pre-symptomatic people, bolstering the need for widespread use of face masks. Centers for Disease Control and Prevention (CDC): This federal agency is the Nation’s top public health agency and is headed by Dr. Robert Redfield, a presidential appointee. The CDC is the lead agency in tracking and responding to epidemics and emerging pandemics. Since the coronavirus is new and was only identified in China in January, the CDC was chiefly reliant upon the WHO for information. The CDC took the WHO’s lead on not recommending face masks for the general public. This became the stance of our federal government during February and March. On April 3, 2020 the CDC announced new guidelines. These new guidelines recommended that the general public should wear nonsurgical cloth face coverings when out in public, when social distancing of 6 feet or more is difficult to maintain (https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/cloth-face-cover-guidance.html). It is important to note that these are recommendations, and there is no requirement to follow them. U.S. Public Health Service (USPHS): This federal agency is headed by Surgeon General Jerome Adams, a presidential appointee. In a February 29, 2020 tweet, the Surgeon General wrote “Seriously people. STOP Buying Masks! They are NOT effective in preventing general public from catching #Coronavirus…”. He reversed course on April 3, 2020 to come in line with the new CDC guidelines. Dr. Anthony Fauci: Dr. Fauci is the director of the National Institute of Allergy and Infectious Diseases (NIAID). Dr. Fauci is a career civil servant and can’t be fired by the president. He serves in an advisory role and is a key member of the president’s corona virus task force. Dr. Fauci has been a clear and reasoned voice on the task force, and during the early months of the pandemic Dr. Fauci was in agreement with the CDC regarding the use of face masks. But he has since admitted that the delay in recommending general mask use was motivated by a desire to conserve dwindling supplies for medical professionals (https://www.thestreet.com/video/dr-fauci-masks-changing-directive-coronavirus). Dr. Fauci is now an ardent supporter of the use of face masks by the general public, and he has often been at odds with President Trump over the government’s response to the coronavirus. President Trump: Even as the CDC and the president’s own coronavirus task force changed their tunes on the use of face masks, the president remained resistant. During the spring and early summer, the president made public appearances in Michigan, Oklahoma, Florida, Arizona, and South Dakota without wearing a face mask, despite local mandates to do so. Many Trump supporters who attended these gatherings modeled the president’s behavior by not wearing face masks. Turning the wearing of face masks into a partisan issue falls squarely on the president. The mocking of Joe Biden for wearing a mask, and refusing to wear a mask in public, was reckless and a failure of leadership. Even the urging of fellow republicans to change his stance, fell on deaf ears. Perhaps Senator Alexander, R-Tennessee said it best, “Unfortunately, this simple, lifesaving practice has become part of a political debate that says: If you’re for Trump you don’t wear a mask. If you’re against Trump you do”. But Alexander’s suggestion that the president set an example for his millions of admirers, did not sway him. According to an Ipsos poll taken in June (https://www.ipsos.com/en-us/news-polls/newsy-COVID-19-June), 60% of Democrats and 34% of Republicans responded that they wear a mask at all times. The poll also reported that 74% of Americans agree that President Trump should wear a face mask in public.  President Trump finally wore a face mask in public on July 11 while visiting Walter Reed National Military Medical Center. But this did not stop the mixed messaging coming from the president and his administration. In an interview with Chris Wallace on Fox News Sunday earlier this month, the president said that he was against a national mask mandate. “No, I want people to have a certain freedom, and I don’t believe in that. No, and I don’t agree with the statement that if everybody wears a mask everything disappears”. By this time the Director of the CDC, the Surgeon General, and Dr. Fauci were practically pleading with the American people to wear face masks in public. The president appears to have finally caught up to his health experts on July 20 when he tweeted a picture of himself wearing a face mask, with the message “We are United in our effort to defeat the Invisible China Virus, and many people say that it is Patriotic to wear a face mask when you can’t socially distance. There is nobody more Patriotic than me, your favorite President!”
Why did the simple act of wearing a face mask become political, and why did the president finally change his tune? President Trump is a politician (although I doubt that he would admit it), and the business of politicians is to get elected and to stay in office. The president is in the middle of a tough reelection campaign, and will often water down the truth and deflect negative news. Prior to the pandemic, President Trump planned to ride his way to reelection on the strength of the economy. As any modern-day politician knows “It’s the economy, stupid”, as coined by Bill Clinton’s campaign strategist James Carville. It is difficult to unseat an incumbent president when the economy is doing well, and it was doing great prior to the pandemic. Unemployment was low and stock market indices were near all-time highs. The global pandemic started to rock financial markets at the end of February, and unemployment began to soar as cities and states began to lock down in March and April. But no matter how much the president tried to ignore the pandemic and wish it away, it only got worse. He simply didn’t want to shine the spotlight on the double-digit unemployment, negative GDP growth, and the financial market turmoil. But what he failed to realize, is that the American people tend to rally behind their leaders in times of crisis, and we are in the middle of a health and economic crisis. Nobody blames the president for the pandemic, just his lack of leadership in the handling of the crisis. If the president showed strong leadership in the face of these two crises, he would be less vulnerable in the upcoming election. It would take several months before the president realized that the new election mantra had become “It’s the coronavirus, stupid”. President Trump could no longer ignore his negative poll numbers. In a July poll by ABC News and the Washington Post, the president’s approval of his handling of the pandemic had fallen to 38%. (https://abcnews.go.com/Politics/64-distrust-trump-coronavirus-pandemic-approval-declines-cases/story?id=71779279). Wearing a facial covering while in public spaces is crucial to slow the spread of coronavirus. But facial coverings are not 100% effective. In order to minimize your exposure, it is also important to maintain social distancing of at least 6 feet, and to practice proper hand sanitation. Wearing a face shield or other eye protection is also recommended when in contact with individuals known, or suspected of having COVID-19. In the next blog post I will explore the different types of face masks and the issue of mask mandates. If you enjoy reading this type of commentary please subscribe to my blog and tell a friend. You will receive an email notification when new blogs are posted. The email will come from the site’s email: [email protected]. To comment click on the blue link below. Thanks, Armchair American |
AuthorThe Armchair American. 
Archives
April 2026
Categories
All
|



 RSS Feed
RSS Feed